VSI Regenerative Medicine

VTFC is now VSI Physical Therapy
Voted ‘Best of Virginia’ 2024
A new name with the same outstanding team and service you can trust.
After two decades of treating patients as “VTFC”, we have revitalized our brand to serve the evolving needs of our patients and align with our parent company Virginia Spine Institute (VSI). We are the same independent physical therapy practice with the same outstanding team, expertise, and offerings we’ve always had. While our name and visual identity have changed, our focus continues to be finding solutions – and Victories – for our patients.
Our licensed orthopedic physical therapists specialize in all areas of the body using modern techniques proven to provide successful outcomes. We provide the highest-quality hands-on physical therapy while using a customized approach for each patient to maximize effective results.
The Ultimate Choice for Ultimate Solutions™️


The knowledge and experience your Physical Therapist has in delivering specific manual therapy techniques can make the difference between success and failure in physical therapy.
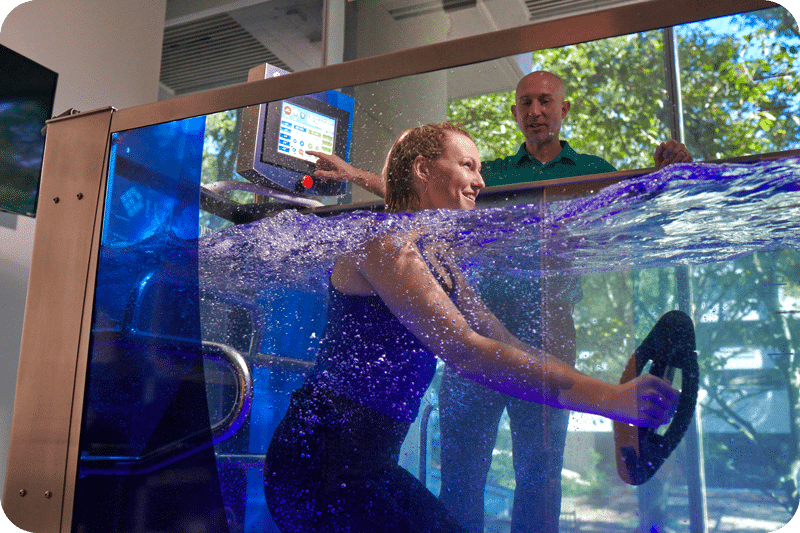
Water serves as a highly effective, nearly weightless environment that offers the ability to improve strength, flexibility, and function to progress recovery.

Dry needling is a technique used to treat myofascial pain syndromes by our team at VSI Physical Therapy, who are all certified in dry needling.

We specialize in working with athletes for both conditioning and rehabilitation purposes. Combining physical therapy, athletic training, and specialized sports massage, we’re here to help you train and meet your goals!

Benefits of
Physical Therapy
At VSI Physical Therapy, we’re more than a physical therapy practice. Our total wellness model treats beyond pain relief and promotes long-term wellness benefits.
Experience the Difference
At VSI Physical Therapy
Patients who experience physical therapy at other practices frequently remark that their experience with us makes an impact on them. We provide the highest level and quality of care in the greater Washington, DC Metropolitan area. At VSI Physical Therapy, we are dedicated to working one-on-one with you and only you! You will have the unique experience of being treated consistently by the same physical therapist(s) for your initial evaluation and follow-up treatments. Each visit is approximately one hour and will include a combination of manual therapy, exercise, and other modalities specifically tailored to your needs.
